Slide 8 of 14
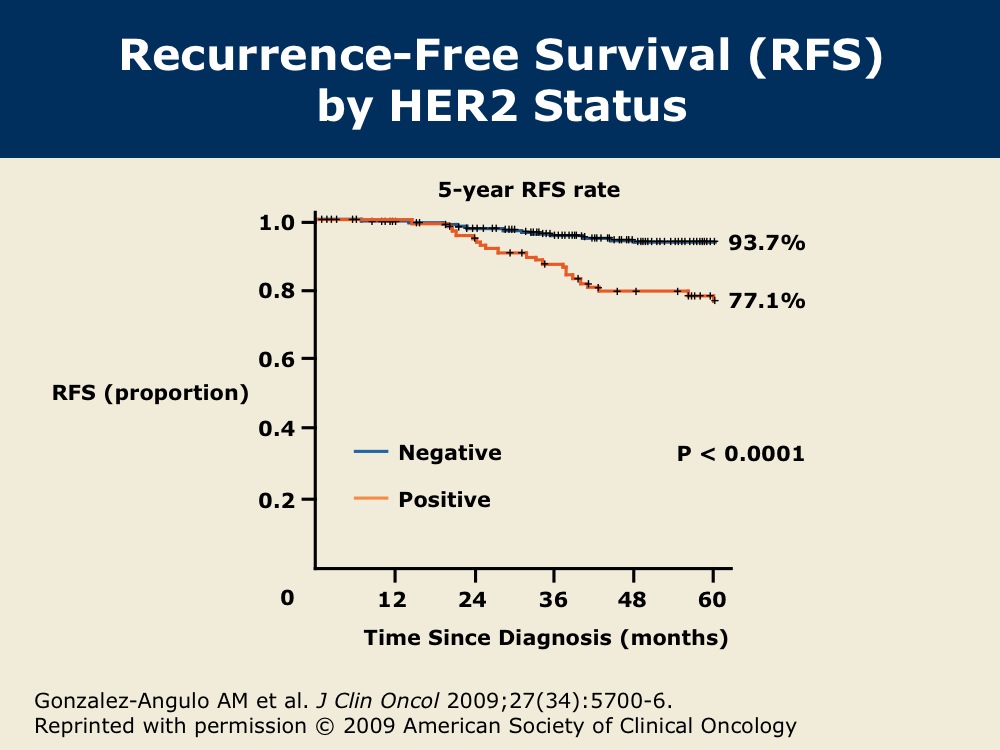
DR GOSS: The question exists as to how to manage clinically early-stage breast cancer that is HER2-positive with small primary tumors. We don’t know the long-term natural history of HER2-positive breast cancer. We know that it’s a marker of early recurrence and higher recurrence risk in both ER-positive and ER-negative breast cancer, but we don’t know the annual hazard of recurrence or the cumulative risk recurrence rate.
The FDA approved trastuzumab initially for patients with node-positive, HER2-positive breast cancer, based on trial results in which the majority of patients had node-positive disease. After the results of the HERA trial the regulatory authorities expanded the indication worldwide to include patients with node-negative breast cancer with tumors larger than one centimeter.
However, many physicians and patients asked: If my tumor is smaller than one centimeter and HER2-positive, what is my risk, and does it merit aggressive therapy with either systemic chemotherapy or anti-HER2 therapy?